Is Zirconia Too Hard or Too Brittle?
What follows is a research-backed breakdown of this common question we get asked about our Prettau Zirconia Bridge. You can find links to all clinical research at the bottom of the page.

What follows is a research-backed breakdown of this common question we get asked about our Prettau Zirconia Bridge. You can find links to all clinical research at the bottom of the page.
You may have heard the claim that Zirconia teeth are “too hard” or “too brittle” and can cause bone loss around implants.
This can sound worrying.
But when we look at the actual clinical research, the evidence tells a very different story.
Multiple long-term studies show that Zirconia implant bridges maintain bone levels just as well, and often better, than acrylic (PMMA) teeth.
In fact, the main difference between the materials is not force on the bone, but how they affect plaque, inflammation, and long-term maintenance.
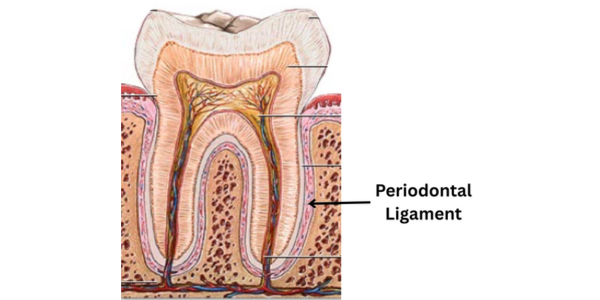
Natural teeth are connected to the bone through a structure called the periodontal ligament (PDL).
This ligament acts like a tiny shock absorber and allows teeth to move slightly when you bite.
Dental implants are different.
They are fused directly to the bone, so they don’t have that same cushioning.
Because Zirconia is a very strong ceramic, some people assume it might put too much pressure on implants.
However, this theory has not been supported by clinical studies.
When researchers follow real patients over many years, Zirconia restorations do not cause increased bone loss.
Both materials are used in implant dentistry, but they behave very differently.
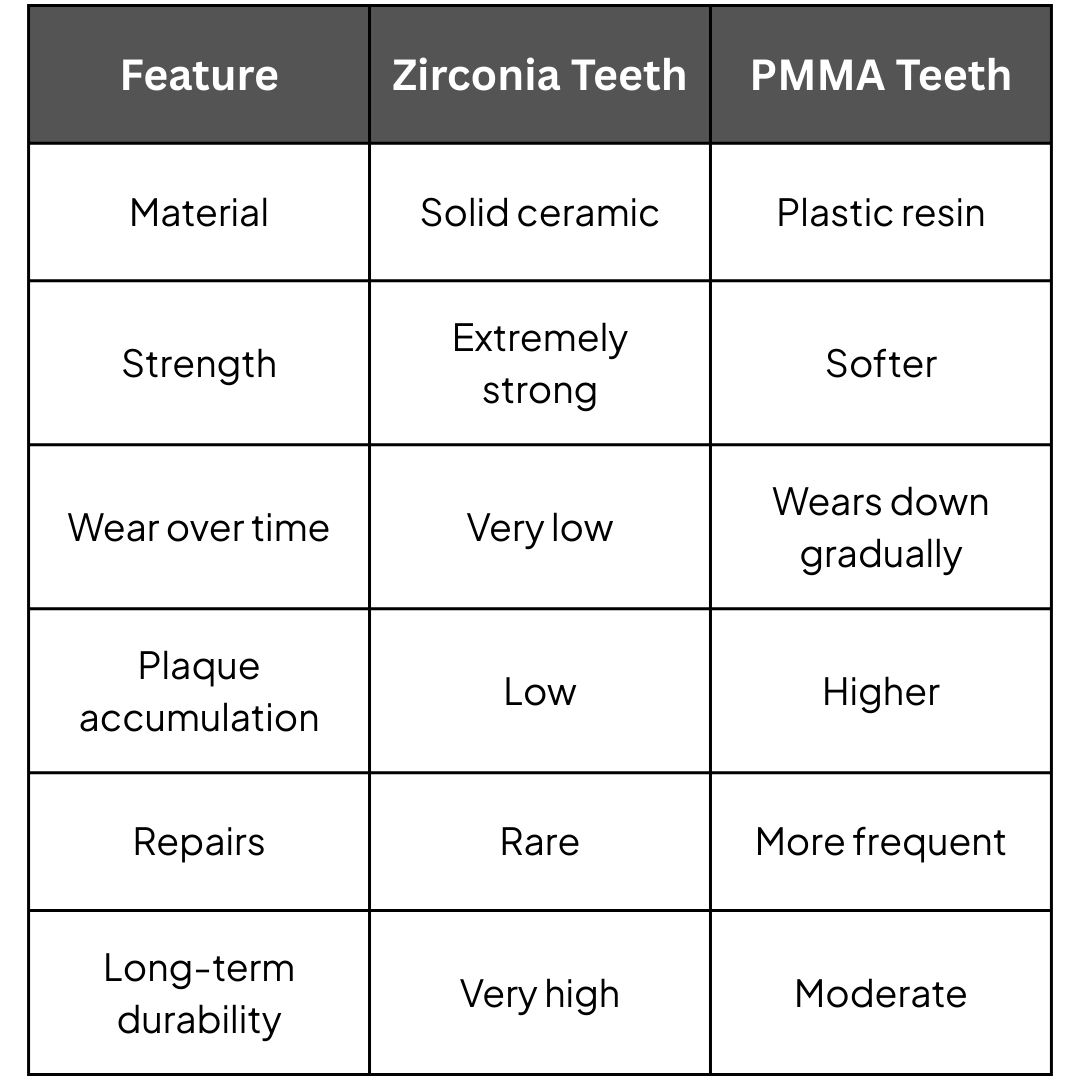
Acrylic teeth are softer and can absorb a small amount of bite force.
But this softness also means they:
Zirconia, on the other hand, is:
This difference in plaque behaviour turns out to be very important for implant health.
Most bone loss around implants is caused by inflammation from bacterial plaque, not mechanical force.
Research consistently shows that:
Because Zirconia has a much smoother surface, it tends to stay cleaner and causes less irritation to the surrounding tissues.
This is one of the reasons many implant centres now consider Zirconia the preferred long-term material.
One of the most important long-term studies followed patients with full-arch implant bridges for six years.
The results were clear:
.png)
Both materials worked.
But the Zirconia group had significantly less bone loss and less plaque accumulation.
This pattern has also been observed in other clinical studies.
Zirconia has become increasingly popular for full-arch implants because it offers:
- Excellent long-term durability
- Very low wear
- Lower plaque accumulation
- Better gum health around implants
-Natural aesthetics
While acrylic restorations can still be used successfully, they typically require more maintenance and replacement over time.
The idea that “Zirconia teeth are too hard or too brittle and cause bone loss” is not supported by scientific evidence.
Long-term clinical research shows that Zirconia restorations:
For these reasons, Zirconia is widely considered one of the most reliable and long-lasting materials for full-arch implant restorations.
"Shock-absorbing concepts for osseointegrated prostheses" by Sompop Bencharit, Root Chumdermpadetsuk et al.
https://digital.car.chula.ac.th/cudj/vol20/iss2/8/
Shock Absorption Capacity of High-Performance Polymers for Dental Implant-Supported Restorations: In Vitro Study
https://www.mdpi.com/2304-6767/12/4/111
Six-year clinical outcomes of implant-supported acrylic vs. ceramic superstructures according to the All-on-4 treatment concept for the rehabilitation of the edentulous maxilla - PMC
https://pmc.ncbi.nlm.nih.gov/articles/PMC8387254/
Zirconia vs. Acrylic Teeth: Which Material Is Best for Your All-on-X Implants?
Implant survival and biologic complications of implant fixed complete dental prostheses: An up to 5-year retrospective study - PubMed
https://pubmed.ncbi.nlm.nih.gov/33618859/

